Nruab nrab mob ntshav qab zib insipidus - kev nkag siab tam sim no ntawm kev kuaj mob thiab kho mob
Ntshav qab zib insipidus (ND) (Latin ntshav qab zib insipidus) - ib qho kab mob tshwm sim los ntawm kev ua txhaum ntawm synthesis, tso pa tawm lossis ua haujlwm ntawm vasopressin, ua kom pom los ntawm kev zam ntawm cov zis ntau nrog ib tus txheeb ze uas tsis muaj (hypotonic polyuria), lub cev qhuav dej thiab nqhis dej.
Phaum Npaum. Kev nthuav dav ntawm ND nyob rau hauv ntau cov pej xeem nws txawv ntawm 0.004% txog 0.01%. Muaj lub ntiaj teb kev coj mus rau qhov nce ntawm ND nthuav dav, tshwj xeeb yog vim nws daim ntawv hauv nruab nrab, uas cuam tshuam nrog qhov nce ntawm cov neeg phais mob ntxiv rau lub hlwb, nrog rau tus lej craniocerebral raug mob, nyob rau hauv cov xwm txheej ntawm ND txoj kev loj hlob li 30%. Nws ntseeg tias ND sib npaug cuam tshuam rau poj niam thiab txiv neej. Qhov xwm txheej siab tshaj tshwm sim thaum muaj hnub nyoog 20-30 xyoo.
Raws tu qauv npe: Ntshav qab zib insipidus
Tus lej (lej) raws li ICD-10:
E23.2 - Mob ntshav qab zib insipidus
Hnub Kev Cai Sawv Cev: Plaub Hlis 2013
Cov tsiaj ntawv siv Siv nyob rau hauv raws tu qauv:
ND - ntshav qab zib insipidus
PP - thawj polydipsia
MRI - sib nqus resonance duab
HELL - ntshav siab
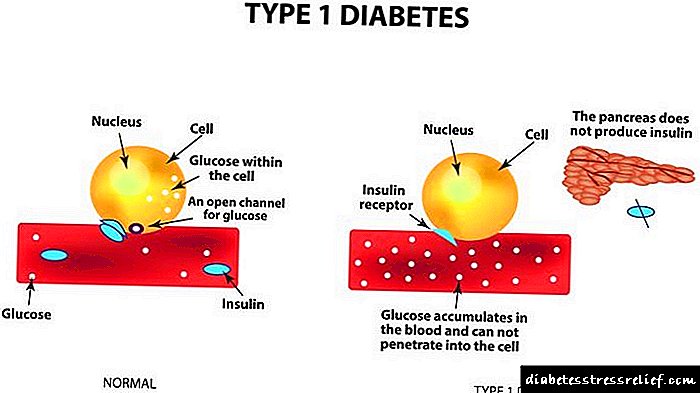
Mob ntshav qab zib mellitus
Ultrasound - Ultrasound
Lub plab zom mov
NSAIDs - cov tshuaj uas tsis yog tshuaj steroidal los tiv thaiv
CMV - cytomegalovirus
Tus neeg mob qeb: cov txiv neej thiab poj niam hnub nyoog 20 txog 30 xyoo, keeb kwm ntawm kev raug mob, kev tiv thaiv mob neurosurgical, hlav (craniopharyngoma, germinoma, glioma, thiab lwm yam), kis mob (kab mob CMV sib kis, toxoplasmosis, encephalitis, mob txha caj qaum).
Cov siv raws tu qauv: cov kws kho mob hauv cheeb tsam, tus kws kho mob endocrinologist ntawm tus kws kho mob polyclinic lossis tsev kho mob, tsev kho mob neurosurgeon, tsev kho mob uas tau txais kev raug mob, tus kws kho mob hauv nroog.
Kev faib tawm
Kev soj ntsuam kev faib tawm:
Feem ntau muaj:
1. Qhov Nruab Nrab (hypothalamic, pituitary), vim qhov tsis hnov lus zoo thiab ua rau vasopressin zais cia.
2. Cov tshuaj nerogenrogen (lub raum, vasopressin - tiv taus), tus cwj pwm los ntawm lub raum tsis kam rau vasopressin.
3. Thawj cov tshuaj tiv thaiv polydipsia: ib qho kev tsis sib haum xeeb thaum muaj kev nqhis dej ntawm lub cev (dipsogenic polydipsia) los yog kev yaum kom haus dej (lub siab polydipsia) thiab kev noj haus ntau dhau ntawm cov dej ua rau lub cev tawm ntawm vasopressin, uas ua rau muaj cov yam ntxwv ntawm cov ntshav qab zib insipidus, thaum vasopress hluav taws xob ua rau lub cev qhuav dej. tab tom raug txum tim rov qab los.
Lwm hom mob ntshav qab zib ua kom ntshav qab zib insipidus kuj paub qhov txawv:
1. Cov tshuaj tiv thaiv kab mob cuam tshuam nrog cov kev ua si ntau ntxiv ntawm cov placenta enzyme - arginine aminopeptidase, uas rhuav tshem vasopressin. Tom qab yug menyuam, qhov xwm txheej ib txwm ua.
2. Kev ua haujlwm: tshwm sim hauv cov menyuam ntawm thawj xyoo ntawm lub neej thiab tshwm sim los ntawm immaturity ntawm lub concentration mechanism ntawm ob lub raum thiab nce kev ua haujlwm ntawm hom 5 phosphodiesterase, uas ua rau muaj kev cuam tshuam sai ntawm cov receptor rau vasopressin thiab lub sijhawm luv luv ntawm kev ua ntawm vasopressin.
3. Iatrogenic: kev siv ntawm diuretics.
Kev faib tawm ntawm ND raws li kev ua txhaum loj:
1. mob me me - tso zis ntau txog 6-8 l / hnub yam tsis muaj kev kho mob,
2. nruab nrab - tso zis tawm txog li 8-14 l / hnub yam tsis muaj kev kho mob,
3. mob hnyav - tso zis ntau dua 14 l / hnub yam tsis muaj kev kho mob.
Kev faib tawm ND raws li kev ua tiav ntawm kev them nyiaj:
1. Nyiaj them rov qab - hauv kev kho mob ntawm kev nqhis dej thiab polyuria tsis txhob thab,
2. subcompensation - thaum kho mob muaj qee ntu kev nqhis dej thiab polyuria thaum nruab hnub,
3. decompensation - nqhis dej thiab polyuria mob siab.
Kev kuaj mob
Cov npe ntawm cov kev kuaj mob tseem ceeb thiab ntxiv:
Kev kuaj mob ua ntej npaj kho tsev kho mob:
- kev soj ntsuam tso zis tawm dav dav,
- biochemical tsom xam cov ntshav (potassium, sodium, tag nrho calcium, ionized calcium, qabzib, tag nrho cov protein, urea, creatinine, ntshav osmolality),
- kev ntsuas ntawm diuresis (> 40 ml / kg / hnub,> 2l / m2 / hnub, osmolality ntawm cov zis, tus txheeb ze ntom ntom).
Cov kev kuaj mob tseem ceeb:
- Qauv nrog kev noj qhuav (kuaj lub cev qhuav dej),
- Sim nrog desmopressin,
- MRI ntawm hypothalamic-pituitary tsam
Cov kev kuaj mob ntxiv:
- raum ultrasound,
- Kev tshuaj ntsuam raum zoo
Kev kuaj mob:
Kev tsis txaus siab thiab anamnesis:
Cov kev tshwm sim tseem ceeb ntawm ND yog polyuria mob hnyav (tso zis ntau dua 2 l / m2 rau ib hnub lossis 40 ml / kg ib hnub hauv cov menyuam yaus thiab cov laus), polydipsia (3-18 l / hnub) thiab cuam tshuam kev cuam tshuam txog kev pw tsaug zog. Qhov kev nyiam rau qhov txias txias / dej khov yog yam ntxwv. Tej zaum yuav muaj cov tawv nqaij qhuav thiab cov leeg ua kua, txo qis ua kom muaj qaub ncaug thiab tawm hws. Qab los feem ntau yog txo qis. Qhov loj ntawm cov tsos mob nyob ntawm lub teeb ntawm neurosecretory tsis txaus. Nrog rau ib feem tsis muaj vasopressin, cov tsos mob hauv kev soj ntsuam yuav tsis meej thiab tshwm sim rau cov neeg tsis haus dej ntau dhau los yog muaj dej ntau dhau. Thaum sau cov anamnesis, nws yog qhov yuav tsum tau hais meej lub sijhawm thiab kev mob siab rau cov neeg mob, muaj cov tsos mob ntawm tus mob polydipsia, mob polyuria, ntshav qab zib hauv cov neeg txheeb ze, keeb kwm ntawm kev raug mob, kev tiv thaiv neurosurgical, qog (craniopharyngioma, germinoma, glioma, thiab lwm yam), kis mob (kab mob CMV sib kis , toxoplasmosis, mob hlwb, mob rau daim npluag qhwv paj hlwb).
Hauv cov menyuam mos thiab menyuam mos, cov duab hauv chaw soj ntsuam kab mob tau sib txawv ntawm cov neeg laus, vim tias lawv tsis tuaj yeem qhia lawv txoj kev xav tau kev muaj dej ntau ntxiv, uas ua rau muaj kev cuam tshuam kev kuaj mob tsis tu ncua thiab tuaj yeem ua rau lub hlwb tsis ua haujlwm. Cov neeg mob no tuaj yeem ua rau poob phaus, qhuav thiab daj ntseg ntawm daim tawv nqaij, tsis muaj lub kua muag thiab tawm hws, thiab qhov nce hauv lub cev kub. Tej zaum lawv yuav xav pub mis niam rau dej haus, thiab qee zaum tus kab mob tsuas yog tsos mob tsuas yog tom qab peb tau menyuam tas. Cov zis osmolality muaj tsawg thiab tsis tshua muaj siab tshaj 150-200 mosmol / kg, tab sis polyuria zoo nkaus li tsuas yog thaum muaj dej nce ntxiv rau me nyuam. Hauv cov menyuam yaus ntawm lub hnub nyoog yau no, hypernatremia thiab hyperosmolality ntawm cov ntshav nrog kev qaug dab peg thiab coma feem ntau thiab sai sai tsim.
Hauv cov menyuam yaus dua, nqhis dej thiab mob polyuria tuaj yeem ua rau pom cov tsos mob hauv kev kho mob, nrog cov kua dej tsis txaus, kev mob tshwm sim ntawm hypernatremia tshwm sim, uas tuaj yeem hloov mus rau tsis nco qab thiab mob plab. Cov menyuam yaus loj hlob tsis zoo thiab muaj qhov hnyav, lawv feem ntau ntuav thaum noj mov, tsis qab los noj mov, mob hypotonic, cem quav, lub hlwb rov qab zoo li tau pom. Tshaj tawm hypertonic lub cev qhuav dej tsuas yog tshwm sim thaum tsis muaj kev nkag mus cuag cov kua dej.
Kev soj ntsuam lub cev:
Ntawm kev kuaj xyuas, pom cov tsos mob lub cev qhuav dej: daim tawv nqaij qhuav thiab cov qog ua kua. Systolic ntshav siab yog qhov qub lossis qis dua, ntshav diastolic ntau zog.
Kev tshawb fawb kuaj:
Raws li kev ntsuam xyuas dav dav ntawm cov zis, nws yog qhov tso tseg, tsis muaj cov kab pathological, nrog tus txheeb ze tsawg tsawg (1,000-1,005).
Txhawm rau txiav txim siab lub peev xwm ntawm lub raum, ib qho kev sim yog nqa tawm raws li Zimnitsky. Yog tias nyob rau hauv ib feem twg qhov tshwj xeeb ntawm kev tso zis ntau dua 1.010, tom qab ntawd kev kuaj mob ntawm ND tuaj yeem raug tshem tawm, txawm li cas los xij, nws yuav tsum nco ntsoov tias qhov muaj piam thaj thiab protein ntau hauv cov zis ntxiv qhov tshwj xeeb ntawm kev tso zis.
Plasma hyperosmolality muaj ntau dua 300 mosmol / kg. Nquag, ntshav plasma osmolality yog 280-290 mosmol / kg.
Hypoosmolality cov zis (tsawg dua 300 mosmol / kg).
Hypernatremia (ntau dua 155 meq / l).
Nrog rau daim ntawv hauv nruab nrab ntawm ND, qhov kev txo qis ntawm qib vasopressin hauv cov ntshav cov ntshav tau sau tseg, thiab nrog rau daim ntawv nephrogenic, nws yog qhov ib txwm lossis nce me ntsis.
Kuaj xyuas lub cev qhuav dej (sim nrog rau noj kom qhuav). G.I. Kev Tshawb Xyuas Lub Cev Muaj Dej Qhuav Robertson (2001).
Theem Dej Qhuav:
- Noj ntshav rau osmolality thiab sodium (1)
- sau cov zis los txiav txim seb lub ntim thiab osmolality (2)
- ntsuas qhov hnyav (3)
- Tswj ntshav siab thiab lub plawv dhia (4)
Tom qab, ntawm kev sib luag ntawm lub sijhawm, nyob ntawm tus neeg mob tus mob, rov ua dua 1-4 tom qab 1 lossis 2 teev.
Tus neeg mob tsis raug tso cai rau haus, nws kuj raug nquahu kom txwv cov zaub mov, tsawg kawg thaum thawj 8 teev ntawm kev kuaj. Thaum pub zaub mov rau cov zaub mov yuav tsum tsis muaj dej ntau thiab yooj yim zom cov khoom noj carbohydrates, hau qe, mov ci, nqaij tsawg, nqaij ntses yog qhov zoo dua.
Tus qauv nres thaum:
- ntau dua 5% ntawm lub cev hnyav
- kev tsis nqhis dej tsis txaus ntseeg
- objectively loj tus mob ntawm tus neeg mob
- kev nce sodium thiab ntshav osmolality ntau dua ib txwm txwv.
Tshuaj Ntsuam Kev Ntshaw DesmopressinCov. Qhov ntsuas yog nqa tawm sai li sai tau tom qab qhov kawg ntawm lub cev qhuav dej, thaum qhov siab tshaj plaws ntawm kev zais / ua hauj lwm ntawm cov vasopressin endogenous tau mus txog. Tus neeg mob tau muab 0.1 mg ntawm ntsiav tshuaj desmopressin nyob rau hauv tus nplaig kom txog thaum ua tiav resorption lossis 10 intg intranasally hauv hom tshuaj txau. Cov zis osmolality tau ntsuas ua ntej desmopressin thiab 2 thiab 4 teev tom qab. Thaum qhov kev kuaj ntawd, tus neeg mob tau tso cai rau haus, tab sis tsis pub ntau tshaj 1.5 npaug ntawm cov zis muaj zis, ntawm kev ntsuas lub cev qhuav dej.
Kev txhais ntawm cov kev sim ua nrog desmopressin: Cov ib txwm los yog thawj cov tshuaj polydipsia ua rau muaj cov zis ntau dua 600-700 mosmol / kg, osmolality ntawm cov ntshav thiab sodium nyob hauv thaj tsam li ib txwm muaj, zoo rau lub cev tsis hloov pauv. Desmopressin xyaum tsis nce osmolality ntawm cov zis, vim nws qhov siab tshaj plaws tau mus txog.
Nrog rau hauv nruab nrab ND, tso zis osmolality thaum lub cev qhuav dej tsis ntau tshaj li ntshav osmolality thiab tseem nyob qis dua 300 mosmol / kg, ntshav thiab sodium osmolality nce, cim kev nqhis dej, hnoos qeev qhuav, nce lossis txo ntshav siab, tachycardia. Nrog kev qhia txog ntawm desmopressin, lub osmolality ntawm cov zis nce ntxiv ntau dua 50%. Nrog nephrogenic ND, lub osmolality ntawm cov ntshav thiab sodium nce ntxiv, cov osmolality ntawm cov zis yog tsawg dua 300 mosmol / kg zoo li nrog ND hauv nruab nrab, tab sis tom qab siv desmopressin, osmolality ntawm cov zis tso tawm tsis nce (nce txog li 50%).
Kev txhais lus ntawm cov txiaj ntsig ntawm kev ntsuas tau muab coj los piav qhia hauv tab. Cov.
Zis osmolality (mosmol / kg) | TUAG | |
| Kuaj xyuas lub cev qhuav dej | Tshuaj Ntsuam Kev Ntshaw Desmopressin | |
| >750 | >750 | Norm lossis PP |
| >750 | ND Nruab Nrab | |
| Neesrogenic ND | ||
| 300-750 | ND ib nrab ntawm ND, ib feem ntawm nephrogenic ND, PP | |
Kev tshawb fawb seev:
ND Nruab Nrab yog suav tias yog lub cim ntawm cov kab mob pathology ntawm hypothalamic-pituitary cheeb tsam. Hlwb MRI yog cov qauv ntawm kev xaiv hauv kev txheeb xyuas cov kab mob ntawm lub cheeb tsam hypothalamic-pituitary. Nrog central ND, hom no muaj ntau yam zoo dua ntawm CT thiab lwm txoj kev kos duab.
Lub hlwb MRI raug siv los txheeb xyuas qhov ua rau hauv nruab nrab ntawm ND (cov qog, mob ua mob rau hauv lub cev, cov kab mob siab ntau ntawm hypothalamus thiab pituitary caj pas, thiab lwm yam.) Thaum mob nephrogenic ntshav qab zib insipidus: kev kuaj ntshav ntawm lub xeev ntawm lub raum kev ua haujlwm thiab ultrasound ntawm lub raum. hauv qhov muaj zog, txij thaum muaj qee kis thaum ND nruab nrab NN tshwm sim ob peb xyoos ua ntej kuaj pom qog
Kev qhia rau cov lus ntuas:
Yog tias pathological hloov chaw hauv hypothalamic-pituitary thaj tsam yog xav tias tsam, kev sab laj ntawm tus kws kho mob hlwb thiab tus kws kho qhov muag tau qhia. Yog tias pom muaj kab mob ntawm cov kab mob tso zis - kuaj mob urologist, thiab thaum paub tseeb tias cov psychogenic variant ntawm polydipsia, kev sab laj nrog kws kho mob hlwb lossis neuropsychiatrist yog qhov tsim nyog.
Synthesis thiab tso pa tawm ntawm antidiuretic hormone
Lub antidiuretic hormone vasopressin yog tsim kho nyob rau hauv supraoptic thiab paraventricular nuclei ntawm hypothalamus. Hu rau neurophysin, qhov nyuaj nyob rau hauv daim ntawv ntawm granules yog thauj mus rau lub davhlau ya nyob twg txuas ntxiv ntawm cov axon ntawm neurohypophysis thiab nruab nrab nce. Hauv cov axon xaus rau qhov kev sib cuag nrog cov hlab ntsha, qhov ntau zuj zus ntawm ADH tshwm sim. ADH tso pa tawm nyob ntawm ntshav ntshav osmolality, cov ntshav ncig thiab ntshav tawm ntshav. Osmotically rhiab hlwb nyob rau thaj chaw ze ntawm thaj chaw anterior hypothalamus hnov mob hloov pauv ntawm cov roj ntsha sib xyaw. Cov kev ua si ntau ntxiv ntawm osmoreceptors nrog kev nce ntshav osmolality stimulates vasopressinergic neurons, los ntawm qhov xaus ntawm uas vasopressin tso tawm rau hauv cov ntshav dav dav. Raws li cov kev mob ntawm lub cev, ntshav osmolality muaj ntau nyob rau ntawm 282–300 mOsm / kg. Nquag, qhov pib ntawm kev zais cia ntawm ADH yog osmolality ntawm ntshav ntshav pib los ntawm 280 mOsm / kg. Cov nqi qis dua rau kev zais cia ntawm ADH tuaj yeem pom thaum cev xeeb tub, mob hlwb, thiab cov kab mob oncological. Kev txo qis ntshav osmolality tshwm sim los ntawm kev nqus ntawm cov kua dej ntau hauv lub cev kom tsis zais ntawm ADH. Nrog plasma ntshav osmolality theem ntawm ntau dua 295 mOsm / kg, ib qho kev nce ntxiv ntawm ADH tso pa tawm thiab ua kom muaj kev nqhis dej ntawm lub chaw nqhis dej tau sau tseg. Lub chaw qhib ua haujlwm ntawm kev nqhis dej thiab ADH, tswj hwm los ntawm osmoreceptors ntawm vascular plexus ntawm sab xub ntiag ntawm hypothalamus, inhibits lub cev lub cev qhuav dej.

Kev cai ntawm vasopressin zais cia tseem nyob ntawm kev hloov pauv hauv cov ntshav. Nrog los ntshav, volumoreceptors nyob rau sab laug atrium muaj qhov cuam tshuam zoo rau kev zais ntawm vasopressin. Hauv cov hlab ntsha, ntshav siab ua los ntawm, uas yog nyob ntawm cov leeg nqaij mos ntawm cov hlab ntsha. Cov nyhuv vasoconstrictive ntawm vasopressin thaum poob ntshav yog vim qhov txo qis hauv cov leeg txheej ntawm cov hlab ntsha, uas tiv thaiv kom tsis txhob poob ntshav siab. Nrog kev txo ntshav siab los ntawm ntau dua 40%, muaj qhov nce ntawm ADH, 100 lub sij hawm siab dua nws cov basal concentration ntawm 1, 3. Baroreceptors nyob hauv carotid sinus thiab aortic arch teb rau kev nce siab hauv cov ntshav siab, uas thaum kawg ua rau txo qis hauv ADH tso pa tawm. Tsis tas li ntawd, ADH yog kev koom tes hauv kev tswj hwm ntawm hemostasis, kev sib txuas ntawm cov prostaglandins, thiab txhawb kev tso tawm ntawm renin.
Sodium ions thiab mannitol yog cov kev txhawb zog ntawm vasopressin zais cia. Urea tsis cuam tshuam rau lub zais ntawm qhov hormone, thiab cov kua nplaum ua rau kev tsis tuaj yeem ntawm nws txoj kev zais.
Tus txheej txheem ntawm kev txiav txim ntawm antidiuretic hormone
ADH yog tus tswj hwm tseem ceeb tshaj plaws ntawm kev tuav dej thiab muab kua dej homeostasis hauv kev sib xyaw nrog atrial natriuretic hormone, aldosterone thiab angiotensin II.
Lub zog muaj txiaj ntsig tseem ceeb ntawm vasopressin yog kev txhawb nqa dej reabsorption hauv qhov sau cov tubules ntawm lub raum cortex thiab medulla tawm tsam osmotic siab gradient.
Hauv cov hlwb ntawm cov hlab ntsha plab hlaub, ADH ua los ntawm (hom 2 vasopressin receptors), uas yog nyob rau ntawm cov txheej txheem nyias nyias ntawm cov hlwb ntawm cov hlab ntim khaws cia. Kev sib cuam tshuam ntawm ADH nrog ua rau kev ua haujlwm ntawm vasopressin-rhiab adenylate cyclase thiab kev nce ntxiv ntawm cov khoom lag luam ntawm cyclic adenosine monophosphate (AMP). Cyclic AMP ua kom muaj protein kinase A, uas ua rau lub zog sib txuas ntawm cov dej channel protein rau hauv apical membrane ntawm cov hlwb. Qhov no ua kom muaj kev thauj cov dej los ntawm cov lumen ntawm txoj kev sib sau mus rau hauv lub cell thiab ntxiv mus: los ntawm cov protein ntawm cov dej ntws nyob rau ntawm cov membrane basolateral thiab cov dej thauj mus rau hauv qhov chaw sib cais, thiab tom qab ntawd mus rau hauv cov hlab ntshav. Raws li qhov tshwm sim, cov zis muaj zog nrog siab osmolality tau tsim.

Osmotic concentration yog qhov tshuaj tag nrho ntawm txhua cov roj yaj. Nws tuaj yeem txhais tau raws li osmolarity thiab ntsuas hauv osmol / l lossis li osmolality hauv osmol / kg. Qhov txawv ntawm osmolarity thiab osmolality cov lus dag hauv txoj kev tau txais cov nqi no. Rau osmolarity, qhov no yog qhov muab xam cov txheej txheem rau qhov tseem ceeb ntawm cov xaim hluav taws xob hauv cov kua ntsuas. Cov lus qhia rau xam osmolarity:
Osmolarity = 2 x Lub osmolality ntawm ntshav, tso zis thiab lwm yam kua hauv lub cev yog lub siab osmotic, uas nyob ntawm tus nqi ions, qabzib thiab urea, uas tau txiav txim siab siv osmometer ntaus ntawv. Osmolality tsawg dua osmolarity los ntawm qhov ntau ntawm oncotic siab. Nrog kev tso cai ib txwm ntawm ADH, tso zis osmolarity yog ib txwm siab dua 300 mOsm / l thiab tseem tuaj yeem nce ntxiv rau 1200 mOsm / l thiab ntau dua. Nrog lub cev tsis muaj peev xwm ntawm ADH, tso zis osmolality qis dua 200 mosm / l 4, 5. Ntawm cov thawj qhov tseem ceeb ntawm txoj kev loj hlob ntawm LPC, ib hom kab mob kev sib koom ua ke ntawm tus kab mob yog kis tau uas yog kis tau los ntawm lossis hom qub txeeg qub teg. Lub xub ntiag ntawm tus kab mob tuaj yeem tshawb nrhiav hauv ntau tiam neeg thiab muaj peev xwm cuam tshuam rau ntau tsev neeg, nws yog vim muaj kev hloov pauv uas ua rau muaj kev hloov pauv hauv tus qauv ntawm ADH (DIDMOAD syndrome). Congenital anatomical kab mob hauv txoj kev txhim kho ntawm nruab nrab thiab diencephalon kuj tseem tuaj yeem ua thawj coj ntawm kev txhim kho ntawm lub hlwb tsis tshua muaj hlwb. Hauv 50-60% ntawm cov neeg mob, qhov pib ua rau tus mob qes qis tsis tuaj yeem tsim - qhov no yog qhov tseem ceeb hu ua idiopathic diabetes insipidus. Ntawm cov theem nrab ua rau muaj kev txhim kho hauv lub hauv nruab nrab cov hlab hlwb, txhawm (mob ntxiv, mob qhov muag, pob txha lov ntawm lub hauv paus txha taub hau) yog hu ua kev raug mob. Txoj kev loj hlob ntawm theem nrab NSD tej zaum yuav cuam tshuam nrog rau cov xwm txheej tom qab transcranial lossis transsphenoidal kev ua haujlwm ntawm lub caj pas pituitary rau cov qog hlwb lub hlwb xws li craniopharyngioma, pinealoma, germinoma, ua rau muaj kev cuam tshuam thiab atrophy ntawm cov posterior pituitary caj pas. Kev hloov pauv ntawm cov mob hypothalamus, mob hnyuv supraopticohypophysial, kev lom zem, ceg, pos sab tom qab ntawm lub caj pas pituitary kuj tseem ua rau lwm qhov kev loj hlob ntawm cov ntshav siab. Lub hauv paus pib ntawm kev tshwm sim ntawm cov qauv organic ntawm tus kab mob yog kis tau. Ntawm cov kab mob kis tau zoo, mob khaub thuas, mob txha caj qaum, mob rau daim npluag paj hlwb, mob txhawm dej, txhab taub hau, txhaws txhaws qa, txhaws txhaws txhaws tau qhov kis, txhawm rau kis mob sib kis - mob ntsws, mob brucellosis, mob syphilis, mob npaws, mob rheumatism 9, 10. Ntawm cov vascular ua rau cov ntshav qis ntawm lub cev neural dysplasia yog Skien's syndrome, cuam tshuam rau cov ntshav tsis txaus rau cov neurohypophysis, thrombosis, thiab leeg pob txha. Nyob ntawm qhov chaw anatomical, LPC tuaj yeem ua chaw ruaj khov los yog hloov chaw. Nrog kev puas tsuaj rau supraoptic thiab paraventricular nuclei, ADH tsis ua haujlwm. Txoj kev loj hlob ntawm nephrogenic ND yog ua raws li cov kab mob ua ntej los yog cov kabmob ua pa ntawm cov hlab ntsha hauv lub raum, uas ua rau lub cev tsis kam ntawm cov receptors rau qhov kev txiav txim ntawm ADH. Hauv qhov no, cov ntsiab lus ntawm endogenous ADH tuaj yeem yog qhov qub lossis nce siab, thiab noj ADH tsis tshem tawm cov tsos mob ntawm tus kab mob. Neesrogenic ND tuaj yeem tshwm sim tau ntev ntev los ntawm mob txeeb zig ntawm tus mob txeeb zig, mob urolithiasis (ICD), thiab prostate adenoma. Cov tsos mob nephrogenic ND tuaj yeem tshwm sim hauv cov kab mob nrog rau kev puas tsuaj rau txoj hlab ntsha hauv lub raum, xws li ntshav liab, mob sarcoidosis, amyloidosis. Hauv cov xwm txheej ntawm hypercalcemia, qhov rhiab heev rau ADH txo qis thiab dej rov txo kom tsawg. Kev mob hlwb psychogenic polydipsia nthuav dav nyob rau ntawm cov leeg hlwb feem ntau yog ua rau cov poj niam tsis muaj hnub nyoog lawm (Cov Lus 1). Qhov pib tshwm sim ntawm kev nqhis dej yog vim kev ua haujlwm tsis zoo nyob rau hauv qhov chaw nqhis dej. Nyob rau ntawm tus ntawm cov kua ntau thiab qhov nce ntawm qhov ntim ntawm cov ntshav ntshav, ib qho kev txo qis ntawm ADH tso pa tawm tshwm sim los ntawm baroreceptor mechanism. Ib qhov urinalysis raws li Zimnitsky hauv cov neeg mob no qhia txog qhov kev txo qis hauv qhov txheeb ze, thaum lub siab ntawm sodium thiab osmolarity ntawm cov ntshav tseem ib txwm lossis txo qis. Thaum txwv cov kua dej kom tsawg, cov neeg mob lub cev tseem zoo txaus siab, thaum cov zis muaj tsawg zuj zus, thiab nws cov osmolarity nce siab ntxiv rau kev txwv lub cev. Rau qhov kev tshaj tawm ntawm ND, nws yog qhov yuav tsum tau ua kom txo qis zais kev muaj peev xwm ntawm cov neurohypophysis los ntawm 85% 2, 8. Cov tsos mob loj ntawm ND yog tso zis ntau dhau thiab nqhis dej heev. Feem ntau cov ntim tso zis ntau dua 5 litres, nws tuaj yeem ncav cuag li 8-10 litres ib hnub. Hyperosmolarity ntawm cov ntshav ntshav txhawb lub plawv nqhis dej. Tus neeg mob tsis tuaj yeem ua tsis tau yog haus dej rau ntau tshaj 30 feeb. Tus nqi ntawm cov kua dej cawv nrog daim ntawv me me ntawm tus kab mob feem ntau ncav cuag 3-5 litres, nrog mob hnyav - 5-8 litres, nrog rau daim ntawv hnyav - 10 liters lossis ntau dua. Cov zis muaj xim; nws cov txheeb ze ntom yog 1000–1003. Nyob rau hauv cov xwm txheej ntawm kev haus dej ntau dhau hauv cov neeg mob, qab los noj mov tsawg, lub plab dhau mus, kev tso zis tsawg dua, txoj hnyuv hloov mus qis qis, cem quav pib. Thaum hypothalamic thaj av cuam tshuam los ntawm kev mob lossis mob tshwm sim, nrog rau ND, lwm yam kev cuam tshuam tuaj yeem pom, xws li kev rog dhau, kev loj hlob pathology, galactorrhea, hypothyroidism, ntshav qab zib mellitus (DM) 3, 5. Nrog kev nce ntawm tus kab mob, lub cev qhuav dej ua rau daim tawv nqaij qhuav thiab cov leeg mos, thiab ua rau muaj qaub ncaug poob. - thiab tawm hws, kev txhim kho ntawm stomatitis thiab nasopharyngitis. Nrog rau lub cev tsis muaj dej txaus, feem ntau tsis muaj zog, palpitations pib nce, qhov txo qis hauv ntshav yog sau tseg, mob taub hau sib zog sai, xeev siab tshwm sim. Cov neeg mob tau mob tsis nco qab, tej zaum yuav ua rau hnov tsw, txhawm chim, muaj lub xeev collaptoid.Etiological yam ntawm central ntshav qab zib insipidus
Cov duab hauv chaw soj ntsuam kab mob ntshav qab zib insipidus





-
Mulberry nplooj rau cov ntshav qab zib: hauv paus thiab kho txiv hmab txiv ntoo
Mulberry hauv ntshav qab zib hom 2: cov txiaj ntsig thiab ua mob rau cov ntshav qab zib Tau ntau xyoo, tsis muaj kev vam meej nrog DIABETES? Lub taub hau ntawm lub koom haum: “Koj yuav xav tsis thoob tias yoojyim kho mob ntshav qab zib li cas los ntawm kev noj tshuaj txhua hnub. ... -

-

-